Immunotherapy in Cancer
Published article on cancer immunotherapy.

Immunotherapy in Cancer
by Josef Issels, MD
Rancho Santa Fe, California, U.S.A.
Published in Explore! Volume 7, Number 6, 1997
Reprinted with permission of Explore Publications, PO Box 1508, Mt. Vernon, WA 98273, U.S.A.
During the five decades of my work, I made a number of observations which I believe may be of great importance for cancer therapy. It is now possible to view the utility and possibilities of immunotherapy from a new perspective, from within the context of an interdisciplinary collaboration.
In my opinion, optimum immunotherapy for cancer entails a nonspecific desensitizing, pro-host management which promotes tissue integrity, resistance and immunity, as well as immune stimulation by nonspecific bacterial reagents and by specific active vaccines.
Collaborative interdisciplinary immunotherapy does not replace conventional measures such as surgery, radiation and chemotherapy, but instead provides a new context in which they may be used within appropriate and complementary parameters to achieve better outcomes with fewer side effects. From this perspective, I predict that the future of cancer medicine lies in a thoughtful cooperation of all specialized fields; this way may hold the promise of substantial increases in the cure rates for advanced cancers.
My "whole-body comprehensive immunotherapy" was developed over forty years of clinical research, in a practice which first saw most patients at the end stages of progressive metastatic malignant disease. Approximately 95% of our patients were admitted after all conventional treatment options had been exhausted.
Overwhelmingly confronted by the extraordinary demands of so many far advanced cases, I faced new challenges for management which went far beyond conventional anti-tumor treatments. My therapy was worked out gradually through comparison of meticulously documented data gathered daily from a large cohort of patients hospitalized for months and followed for years.
Guided by Kussmaul's dictum, "the result at the sick-bed is decisive," I searched for ways to restore the body's own natural defenses.
In 1953, I published the "whole body concept" to summarize my observations to date. I placed great emphasis, in addition to anti-tumor treatments, on restoration of the body's own natural defenses and healing mechanisms. Modern research continues to bear out this concept. For humans, as well as for most other vertebrates, the daily random generation of malignant cells represents a chronic challenge (Thomas, Eugster). However, the body's own natural defenses are normally able to prevent randomly generated malignant cells from becoming tumors.
Of all the natural defenses, the T-cell mediated immunities are by far the most sensitive to foreign or abnormal antigens. Also known as the "self/not-self recognition mechanism," the T- cell mediated immunities defend us against bacteria, fungi, viruses and other foreign agents. Responsible for maintaining healthy, normal homeostasis, T-cell mediated immunities also provide constant "immune surveillance" against malignant cells (Thomas).
In other words, our natural defenses include a healthy immune system which protects us against negative elements from the outside environment, and protects the integrity of our internal milieu. In contrast, if the immune system itself is unhealthy, random malignant cells may slip through its surveillance to form the basis of tumors.
Historically, cancer treatments have been mostly restricted to efforts aimed at removing or destroying tumors. My "whole-body comprehensive immunotherapy," of course, also includes direct anti-tumor measures, and in some serious cases I have found that strategically timed low-dose chemotherapy can be lifesaving. But whole-body comprehensive immunotherapy goes far beyond strictly anti tumor treatments to address two sets of causative factors, 1) those which suppressed anti-cancer immune surveillance and 2) those which caused normal cells to become malignant in the first place. Our natural defenses are comprised of an integrated set of enormously complex and specialized systems which continually interact and which are found in virtually every tissue throughout our bodies (Buttersack, Schade, Eppinger).
Schmid and Luckey have defined four integrated "defense zones" (Table 1).
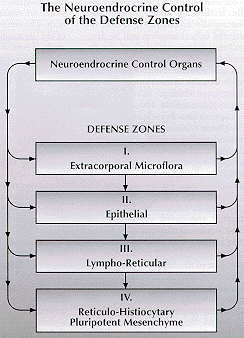
- ● Extracorporal. This zone is made up of "healthy flora" found on many epithelial surfaces, i.e., the point of contact with either the external or the internal environment. These microbes, also known as obligate symbionts, are essential to the normal activity of many epithelial tissues. Healthy flora help enable the body to adapt to changes in its external and internal environments by contributing greatly to the "basic immunity of the Organism" (Gordon, Luckey, Miyakawa), and can be said to protect the other defense zones as well.
- ● Epithelial. This zone is comprised of the skin, the linings of every serous membrane (pericardium, pleura, peritoneum) and mucous membrane (sinuses, lungs, gut), as well as the linings of every duct, gland, cavity, and excreting passage channel and tube in the body. Epithelial cells function to protect, adsorb, filter and excrete, as well as to move substances through ducts, to receive stimuli, and to produce germ cells. In cancer, the elimination of metabolic and tumor-related toxins depends on the normal functioning of epithelial cells. If they are unable to eliminate these rapidly accumulating toxins, the epithelial cells themselves will be damaged and, subsequently, all of the defense zones will be negatively affected.
- ● Lympho-reticular. This zone is a body wide network of fixed and mobile cellular tissue which provides defense by macrophage activity and immunologic mechanisms. It includes the entire lymphatic system, as well as the reticuloendothelial system of monocytes and macrophages found in high concentrations in the reticular tissue of the liver (Kupffer's cells), Waldeyer's tonsillar ring, Peyer's patches, the spleen, the vascular system, the brain, the mucous membranes, and alveoli. Highly specialized retothelial cells which make up the outer linings of reticular tissue, such as white bone marrow and the spleen's white pulp, are also part of this zone. The ability of this network to phagocytize abnormal or aged cells, pathogens, foreign substances, and metabolic by-products has been demonstrated by many authors (Alexander, Good, Hellstrom, Klein, Nossal, Old).
- ● Reticulo-histiocytary. The most massive of the defense zones, it is also referred to as the pluripotent mesenchyme and consists of the connective tissues which support and unite other tissues and structures and account for nearly half of the body's weight. The connective tissues are very vascularized (with the exception of cartilage) and include bone, reticular tissue, adipose tissue, mucous tissue and fibrous tissue (white, yellow, elastic, and areolar). These tissues contain relatively few cells and are largely comprised of the fluid, semi fluid, and solid intercellular matrix, also known as ground substance, whose properties vary with each specific type of connective tissue.
According to Pischinger, the "regulatory ground system" is responsible for: 1) pluripotent hemopoietic precursor cell function and subsequent formation of all types of blood cells, 2) transit functions allowing communication and cooperative interactivity of nerves, organs, blood cells, the lymph system and the gut, 3) maintenance of homeostasis, i.e., protection of the internal milieu, 4) defense, 5) detoxification, and 6) storage, both of toxins and nutrients.
In addition to their role in the body's natural defenses, these four interrelated zones-importantly, under neuroendocrine control-perform many functions which are vital to the homeostasis of the body. The entire natural defense potential of the organism can be suppressed, indirectly, if even one zone is blocked in only one of its functions, e.g., the excretions managed by epithelial cells of zone 2.
The four defense zones act in cybernetic synergy to create what Pischinger calls "die grosse Resistance," or metaresistance. Metaresistance extends far beyond the extensively studied activities of T cell and B cell immunities. Metaresistance is, in essence, a whole-body phenomenon; therefore it must be seen "holistically," a term suggested by the great statesman and philosopher, Jan Christian Smuts, to acknowledge that a living organism must be viewed as a whole and is not reducible to the sum of its parts.
Importantly, the defense zones are under neuroendocrine control. (In fact, recent evidence demonstrates that zone four adipose tissue itself is a type of hormone-producing endocrine tissue.) A disruption of neuroendocrine control centers such as the autonomic nervous system, or the diencephalon (e.g., hypothalmic regulation of hormone release or inhibition, water balance, fat and sugar metabolism, and temperature), can block the functions of the zones and, at the same time, suppress metaresistance. Logically, treatment to restore metaresistance must address these control centers in addition to each of the zones.
Treatment to restore metaresistance must comprehensively address the entire etiological development of disease, i.e., all causative and contributing factors. In my clinical efforts to accomplish this, I came to view the malignant tumor as the product, not the cause, of a definable chronic diseases multi-stage preneoplastic syndrome. Gradually, I cataloged every possible etiological component, including even prenatal factors, and put them into chronological order over the life of the patient. The product of this exercise is formally called the Issels Hypothesis of the Pathogenesis of Cancer (Table 2).
Table 2.
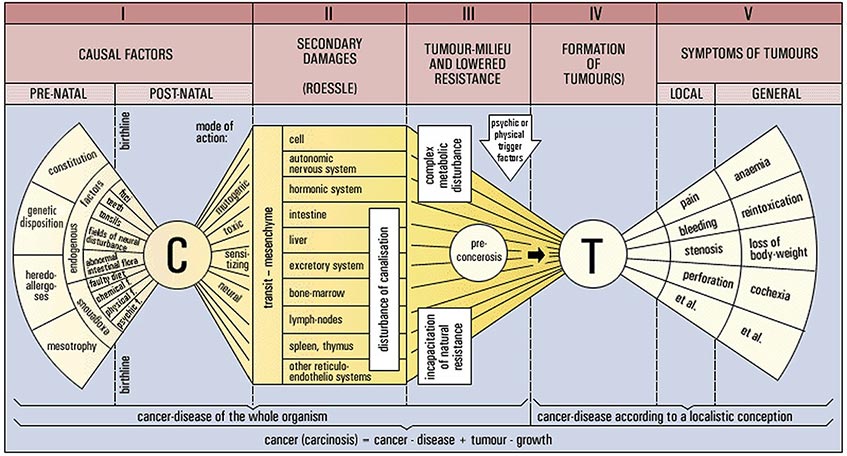
Diagram reprinted by permission. First published in 1953, this version of the diagram was more recently published in Issels J. Immunotherapy in progressive metastatic cancer. Clinical Trials Journal. I970;7(3):357-366.
Prenatal and postnatal causal factors and primary damages (1) indirectly exert chronic negative influences on organs and entire systems by way of their effects (toxic, mutagenic, sensitizing, neural) on the matrix, or ground substance, of the transit mesenchyme, leading to serious disturbances of the neural, hormonal and excretory defense functions, pathological changes called secondary damages (11). The simultaneous and systemic disruption of detoxification which accompanies these pathological changes is a common denominator among all chronic diseases. Disturbed detoxification leads to deterioration of the milieu interior (111), the internal environment comprised of the extracellular fluids. Following deterioration of the milieu are well known and complex metabolic disturbances which are common to all chronic diseases but vary according to normal biodiversity from one individual to another.
Each stage of the cancer syndrome is chronic and additive, so that the primary damages and causal factors of stage one (1) continue even as the secondary damages of stage two (11) develop. The combined effects of primary damages plus causal factors plus secondary damages, including disturbed detoxification, lead to deterioration of the milieu, a consequent failure of the natural defenses, and sometimes pre cancerous lesions (111), all of which in turn are added to the already existing chronic challenges. Finally, the tumor arises (IV) with its own abnormal milieu and symptoms (V). Tumor genesis may or may not be preceded by pre cancerous lesions at the site of least physiological resistance, and may or may not involve a triggering factor. The "localistic" approach views the tumor as the beginning of a disease which progressively spreads throughout the body. In contrast, the holistic model sees cancer as a constitutional malady with the tumor presenting as a late stage symptom.
I concluded from this complex process that oncogenesis consists of four developmental stages which occur in succession and which persist even after the tumor presents. The first three stages represent the latent phase of the cancer syndrome, with stage one consisting of causal factors and primary damages, stage two the development of secondary damages, and stage three suppression of resistance and the establishment of the pre tumor milieu. In stage four, finally, we see the development of the tumor and the establishment of its own abnormal milieu.
Therefore, in the Issels Hypothesis of the Pathogenesis of Cancer, this complex set of pathological influences underlying a chronic condition which culminates in the production of malignant diseases is called "the cancer syndrome" (previously, Krebs-Krankheit or "cancer-disease"). The cancer syndrome is the precondition for the growth of tumors and metastases. This is consistent with Smuts' concept of "holism."
There are many potential prenatal and postnatal causal factors and primary damages which indirectly exert chronic negative influences on organs and entire systems by way of their effects (toxic, mutagenic, sensitizing, neural) on the matrix, or ground substance, of the transit mesenchyme. In addition, these toxic influences may lead to serious disturbances of the neural, hormonal and excretory defense functions, pathological changes which have been dubbed "secondary damages" (Rssle).
The simultaneous and systemic disruption of detoxification which accompanies these pathological changes is a common denominator among all chronic diseases. Disturbed detoxification leads to deterioration of the milieu interior, the internal environment comprised of the extra cellular fluids. Following deterioration of the milieu are well known and complex metabolic disturbances which are common to all chronic diseases but vary according to normal biodiversity from one individual to another.
Each stage of the cancer syndrome is chronic and additive, so that the primary damages and causal factors of stage one continue even as the secondary damages of stage two develop. The combined effects of primary damages plus causal factors plus secondary damages, including disturbed detoxification, lead to deterioration of the milieu and subsequent failure of the natural defenses, which in turn is added to the already existing chronic challenges. Finally, the tumor arises. Tumor genesis may or may not be preceded by pre cancerous lesions at the site of least physiological resistance, and may or may not involve a triggering factor.
One can say that the body has developed a tendency to produce tumors.
This holistic view is quite different from the conventionally accepted "localistic" model, but it is of tremendous importance because it leads to vast improvements in the outcomes of cancer management. In short, the physician is now confronted by two very different, even competitive, paradigms of cancer diagnosis and treatment.
The holistic model, in which cancer is seen as a constitutional malady with the tumor presenting as a late stage symptom, is actually quite consistent with contemporary molecular biological research findings. However, conventional cancer treatment is generally paradigmatic of the older localistic approach and does not reflect new molecular biology findings because no practical applications have yet been developed from this basic research.
The localistic approach views the tumor as the beginning of a disease which progressively spreads throughout the body. This view fosters the illusion that anti-tumor measures alone can be comprehensive and definitive treatment against the "cause" of the disease, which in the localistic approach is the tumor itself. This persistent belief is, in my opinion, the central reason for lack of progress in the war against cancer. Until the cancer establishment acknowledges the cancer syndrome (i.e., chronic causal factors, primary and secondary damages, suppressed natural defenses, etc.), and treats these influences accordingly, in addition to treating the tumor, it is doomed to recreate its own history of vanishingly small numbers of actual cures, as well as the numbing predictability of recurrence in the vast majority of patients with advanced cancers.
Whole-body comprehensive immunotherapy is, by definition, a holistic approach which regards restoration of metaresistance as equal in importance to anti-tumor measures. Therefore, this approach treats causes and chronic damages in order to restore natural immunities and resistance, while at the same time managing the symptoms of the cancer syndrome including, of course, the tumor itself. Both moieties, pro-host treatments and anti-tumor measures, are indispensable; neither one used in isolation will approach the level of success possible with the combination.
The Issels Hypothesis of the Pathogenesis of Cancer is a template for guided interdisciplinary diagnosis and treatment of the cancer syndrome, its underlying contributing influences, and the malignant disease to which it has led.
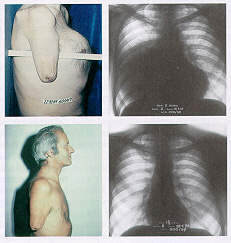
 Patient H.B. 597/66
Patient H.B. 597/66
Complete remission of infiltrating inflammation recurrence of solid Breast Carcinoma by comprehensive immunotherapy without chemotherapy.
No further relapse, no further treatment. Observation 13 years.
 Patient K.W. 600/69
Patient K.W. 600/69
Complete remission of recurrence of huge solid mediastinal malignancy by immunotherapy and two initial shots of chemotherapy.
No relapse, no further treatment for 28 years.
There are three general areas of prohost clinical management which are interwoven, and which overlap considerably:
- Correction of all known causal factors. This requires surgical elimination of foci of infection (notably head foci of dead teeth and nonfunctional diseased tonsils), immunization against pathogenic microbes and administration of appropriate flora, desensitization of local tissue pathologies caused by neural referral of disturbances from distant disease foci (Huneke), treatment of toxicoses and sensitivities caused by inherited latent phase cell wall deficient microbial forms (stemming from ancestral exposure to infections including syphilis and tuberculosis), which are passed on at birth and can persist for many generations (Enderlein, Spengler), replacement of pathogenic nutrition with a dietotherapy specifically designed to meet the special needs of cancer patients (Gerson, Hildenbrand), removal of environmental and psychological stressors as defined by Hans Selye, and the establishment of a more beneficial mind/body homeostasis according to the findings of psychoneuroimmunology.
- Desensitization to causal factors. This is accomplished by systematic autogenous vaccination, application of microflora preparations and various specific vaccines.
- Normalization of secondary damages to the host metabolism (impaired detoxification with subsequent suppression of natural defenses). Treatments include Gerson's dietotherapy, correction of the acid-base balance by treatment of the serum alkalosis and tissue acidosis paradox common in degenerative diseases, hyperthermia, fever therapy (Coley-Nauts), hyperbaric oxygen, ozone, ultraviolet blood irradiation, enzymes, glandulars, organ extracts, and neural therapy (Huneke).
Pro-host treatments are nontoxic and must be applied for many months in order to allow establishment of a durable improvement in the natural defenses.
Conventional anti-tumor treatments (surgery, radiation, chemotherapy) can be utilitarian and beneficial when modified to support the goals of whole-body comprehensive immunotherapy. In this context, they may be used concomitantly with vaccines, dietotherapy, and other host-protective medical measures. Dosages and duration of treatment with these drugs may be far less than is recommended in the randomized clinical trial protocols by which they achieved regulatory approval, but these modifications are justified by the outcomes of my patients, who achieve quite satisfactory tumor response without the typical side effects of hair loss, bone marrow suppression, and gut disturbances.
I have had extensive experience with several immunizing vaccines which promote immune mediated tumor regressions, and have gathered years of cornparative data. Both an autogenous vaccine which I developed, and the pooled mycoplasm preparation of Gerlach (discussed in my earlier publications) consistently produced favorable results.
Clinical experience has shown that advanced cancers, including the leukemias, may undergo complete remission in response to vaccination by tumor antigens given in conjunction with potent appropriate pro-host management. Aggressive application of similar tumor antigen preparations as sole treatment has produced disappointing results in advanced cancers, leading some authors to conclude erroneously that immunization is impossible when the tumor load becomes quite large.
Tumor antigens should not be given in a therapeutic vacuum, but must be supported by treatments which address the suppressed immunological status and defense functions of the advanced cancer patient. Immune incompetence secondary to intoxication caused by neuroendocrine dysfunction can be ameliorated within days after elimination of foci of infection (especially dental and tonsillar) and/or application of fever therapy (Coley).
Early on in the development of my therapy, I became convinced that the ability of the patient to respond to immunotherapy is a function subordinate to the systematic elimination of all known causal factors coupled with appropriate management of both primary and secondary damages. To summarize, it is my opinion that therapeutic detoxification of the tumor milieu potentiates all immunotherapeutic measures and produces consistently better clinical outcomes.
Therapy to restore, maintain, and protect the detoxification mechanisms of the defense zones is not a component of standard conventional cancer managements, but it is of vital importance. Detoxification is central to the success of both cytotoxic drugs and vaccinations. Without adequate detoxification, even when tumors are being destroyed, toxic byproducts of oncolysis may irretrievably overwhelm the host.
Patients endangered by rapidly progressive disease may require treatment with cytotoxic drugs to stop tu- tu growth long enough to establish a response to concomitant immunotherapeutic measures. In our clinical experience, cautious short term administration of chemotherapy avoided the severe immune suppression associated with chronic use of these drugs, a finding consistent with those reported by Frei. Concomitant pro-host measures further reduce this unwanted side effect. I believe that combined prohost, antitumor and immunotherapeutic measures, as embodied in whole-body comprehensive immunotherapy, provide additional hope for the successful management of advanced cancer.
If broadly adopted and applied in appropriate complementary balance, these measures will certainly cure many advanced patients who will otherwise be lost, no matter which monotherapy they receive, nor how aggressively it may be administered. In my experience with the combined treatment, it is not unusual for inoperable tumors to regress enough to be safely removed surgically. I have seen blocked ureters clear, and obstructed biliary systems open up, averting tragedy and allowing further treatment.
In current conventional practice, chemotherapy and radiation are considered appropriate follow-up treatment for surgery, in spite of their well known suppression of the natural defenses. In my experience, many more patients have been cured since the development of whole body comprehensive immunotherapy as the follow-up treatment of choice for any direct anti-tumor measure, whether it be surgery, radiation, chemotherapy, or a potent alternative such as that recently published by Danopoulos, et al. Even though direct measures may completely kill the tumor, only systematic therapeutic restoration of the natural defenses can prevent recurrence by curing the body's pathological tendency to produce tumors. This conviction is bolstered by the long term disease-free and treatment-free survivals of many of my whole-body patients. Some of my patients who were treated for advanced adult cancers during the late 1940s and early 1950's are still alive, having never suffered a recurrence and having required no further treatment for more than forty years.
In 1970, we published data in Clinical Trials Journal (Issels) on 370 patients who were operated or radiated with intent to cure, and whose follow-up treatment was whole-body comprehensive immunotherapy according to the Issels Hypothesis of the Pathogenesis of Cancer. At the time of the publication, 322 (87%) were alive beyond five years and completely free of disease (Table 3). The world statistic for patients in comparable databases is a So% disease-free five year survival rate.
These rates were not statistically compared in the original article, so I offer the following analysis: The survival rate of 87% in a sample of 370 patients has a sampling error of ±1.7%. Using a normal distribution function, k, Of 2.58 we find that the 99% confidence interval for this survival rate is 82.6% – 91.4%. Because the reported world rate Of 50% falls outside of the confidence interval, the 87% observed disease-free five year survival rate for patients treated with whole-body comprehensive immunotherapy is statistically very significant (P < .01).
As early as 1959, an independent retrospective epidemiological review of our charts published in Die Medizinische (Audier) found that 16.6% Of 252 exhaustively pretreated, terminal patients were cured by the whole-body approach. A subgroup of 88 charts of patients with three cancers (breast, colorectal and uterine) was selected for comparison with suitable databases. Of these 88 patients, 27 (31%) achieved durable complete remissions of at least five years. Comparable databases revealed only 7 cures in a sample Of 78 patients (9%). The comparison is statistically significant (chi-square = 7.004 with 1 degree of freedom; P = 0.008).
In 1971, it was reported in General Practitioner (Anderson) that 17% of 570 far advanced whole body patients were disease-free at five years compared to a world statistic of 2%. The sampling error of a 17% cure rate in a sample of 570 is ±1.6%. Using a normal distribution function, k of 2.58, the 99% confidence interval, the comparison is again statistician quite significant (P < .01).
It is important to point out once again that these findings do not suggest that immunotherapeutic and pro-host measures can replace conventional treatments. On the contrary, they offer hope that these conventional tools may yet find greater utility in the context of structured interdisciplinary collaboration.
Each of the component treatments must be administered as a carefully integrated part of the whole clinical approach. It is not enough to offer even the most potent of treatments, whether they be dietotherapy (Gerson, Hildenbrand) or tumor antigens (Issels), without concomitant alleviation of causal factors (e.g., head foci of infections), reversal of primary and secondary damages, correction of the milieu interior, and restoration of the natural defenses.
I am quite aware that the individual pro-host, anti-tumor and immunizing treatments I have discussed here require further development. There is a great need for basic research. But I want to emphasize that it was the guiding concept of "holism" which led me, through development of my Hypothesis of the Pathogenesis of Cancer, to the therapeutic strategy which produced the above massive survival advantages for advanced cancers of all types. And it is this sort of rigorous and systematic interdisciplinary diagnosis and treatment strategy which, if thoughtfully and widely applied, will most certainly lead to higher survival rates in advanced cancer throughout the world.
It has been nearly forty years since the publication of the first independent review of my records, confirming my claim to have discovered a new way to improve the outcomes of cancer management. In spite of the fact that the official "war on cancer" has been stalemated for decades, the cancer establishment remains functionally unaware of these expanded possibilities. With the notable exception of recent renewed, but limited, interest in vaccines, the last three decades have not produced the long awaited breakthroughs in conventional management. Basic research in cancer immunology has thus far resisted translation into meaningful clinical gains. It is the patients who must suffer through routine treatments without any real hope of cure. So much more could be done for them if practitioners were to employ treatments aimed at restoring the natural defenses.
My whole-body comprehensive immunotherapy offers a number of new therapeutic options for prevention of cancer in persons known to be at risk (genetic predisposition coupled with environmental challenges) and for treatment of precancerous lesions. It is also useful as a preparatory treatment to enhance the anti-tumor effects of conventional surgery, radiation, chemotherapy, etc., and it is an essential follow-up treatment for these same procedures. In addition, with collaborative interdisciplinary treatment, it is possible to offer hope to patients for whom even the most aggressive monotherapies are likely to be of little or no value.
Conventional anti-tumor treatments can become useful components of complementary management. As monotherapy, however, even combinations of the most potent conventional anti-tumor treatments cannot cure the patient's cancer syndrome, i.e., the tendency to produce tumors. For this reason, conventional anti-tumor treatments should no longer dominate medical practice to the point of exclusion of complementary managements. Through interdisciplinary collaboration, conventional anti-tumor treatments can be put in a proper context, and their usage can be modified accordingly. By opening the door to cooperative interaction among all appropriate disciplines, we can see our way forward toward the goal we share in common, to rescue more lives from the cancer epidemic.
References:
- Alexander P. In: Prog Emp Tumour Res. 1968; Basel and New York; Karger; 10:22.
- Anderson J. General Practitioner. 1971; March 26:15-16.
- Audier AG. Immunotherapie metastasierender Malignome. Die Medizinische. 1959; 40:1860-64.
- Bahnson CB, et al. Die Bedeutung des eigenen Abwehrvermögens bei der ätiologie malig
- Boyse EA, Old LJ. In: Smith RT, Landy M, eds. Immune Surveillance. 1971; New York: Academic Press.
- Brunner KW, Nagel GA. Internistische Krebstherapie. 1976; Berlin:Springer.
- Burnet M. Immunological Surveillance. 1970; Oxford:Pergamon.
- Buttersack F. Latente Erkrankugnen des Grundgewebes. 1912:Stuttgart.
- Coley-Nauts H, Swift WE, Coley BL. Treatment of Malignant Tumors by Bacterial Toxins. Cancer Research. 1946; 6:205-215
- Crabbe PA, Carbonara AO, Heremans F. The normal human intestinal mucosa as a major source of plasma cells containing yA-immuno-globulin. Lab Invest. 1965; 14:235
- Danopoulos ED, Danopoulou IE. Eleven years experience of oral urea treatment in liver malignancies. Clin Oncol. 1981 Dec; 7(4):281-9.
- Danopoulos ED, Danopoulou IE. The effects of urea treatment in combination with curettage in extensive lip cancers. J Surg Oncol. 1982 Mar;19(3):127-31.
- Enderlein G. Bakterien-Cyclogenie. 1925: Berlin:Walter de Gruyter.
- Eugster J, Hess VF. Die Weltraum-Strahlung und ihre biologische Wirkung. 1940:Zurich.
- Frei E. Combination Cancer Therapy. Cancer Research. 1972; December; 32:2593-2607.
- Gerlach F. Krebsund obligater Pilzparasitismus. 1948; Vienna:Urban and Schwarzenberg.
- ----------. Die Mycoplasmen-Infektion bei Geschwulstkrankheiten des Menschen und der Tiere. Krebgeschehen. 1972; 4:1-4.
- Gerson M. A Cancer Therapy: Results of Fifty Cases. 5th Edition. San Diego, CA; Gerson Institute 1990.
- Gerson M. Effects of combined dietary regime on patients with malignant tumors. Exper Med Surg. 1949;7:299-317.
- Gerson M. No cancer in normal metabolism: Outcomes of a specific therapy. Med Klin. 1954:49(5):175-179: Cancer, a problem of metabolism. Med Klin. 1954: 49(26):1028-1032; On the medications of cancer management in the manner of Gerson. Med Klin. 1954; 49(49):1977-1978.
- Good RA. In: Bergsma D. Immunologic deficiency diseases in man. 1968; New York; Nat'l Fdn March of Dimes:355.
- ----------, Finstad J. Essential Relationship between the lymphoid system and immunity. In:Miescher PA and Graber P, eds. Immunopathology V. 1967.
- Hellström KE and Hellström I. Advan Cancer Res. 1969; 12:167-223.
- ----------. Immunity of Neuroblastoma. Annual Review of Medicine. 1972:23.
- Helm F and Klein E. Arch Dermat. 1965:91(124).
- Hildenbrand GLG, Hildenbrand C, Bradford K, Cavin S. 5 year survival rates of melanoma patients treated by diet therapy after the manner of Gerson. Alt Ther Health. Med. 1995; I(4):29-37.
- ----------, Hildenbrand C, Bardford K, Rogers D, Straus C, Cavin S. The role of follow-up and retrospective data analysis in alternative cancer management: the Gerson experience. J Naturopath Med. 1996; 6(I):49-56.
- ----------, Hildenbrand C, Defining the role of diet therapy in complementary cancer management: prevention of recurrence vs. regression of disease. Proceedings of the First Annual Alternative Therapies Symposium: Creating Integrated Healthcare. January 18-20, 1996, San Diego, CA
- Huneke F. Das Sekundenphänomen. 1956; Ulm and Heidelberg:KF Haug.
- Issels JM. Therapeutische Richtlinien bei inoperablenmalignen Tumoren. Vortrag auf dem 5. Berchtesgadener Kurs f, r Ganzheitsmedizin. 1952. In: Zabel W. Ganzheitsbehandlung der Geschwulstkrankheiten. Stuttgart: Hippokrates.
- ----------. Ergebnisse und Erkenntnisse nach vierjähriger klinisch-interner Therapie beim inkurablen Krebskranken. Hippokrates. 1954; 25 u. Bildbeilage:514-529.
- ----------. Gedanken zur Internen Behandlung von Tumorkranken. Hippokrates. 1956; 27 u. Bildbeilage:173-180.
- ----------. Fokalinfekt und Krebs. Dtsch Zahnärztl Zeitschr. 1956;11:123-131.
- ----------. Mehr Heilungen von Krebs. 1972; Bad Homburg v. d. H. :Helfer.
- ----------. Cancer: A Second Opinion. 1975; London:Hodder and Stoughton.
- ----------. Immunotherapy in progressive metastatic cancer. Clinical Trials Journal. 1970;7(3):357-366.
- Klein G. Tumor Antigens. Ann Rev Microbiol. 1966; 20:233-252.
- Lewis MG, Lewis, TM. Einfluss humoraler Immunmechanismen auf die Metastasierung menschlicher Tumoren. M, nch Med Wchnschr. 1977;28(43):119.
- Luckey TD. Germfree life and gnotobiology. 1963; New York and London:Academic Press.
- ----------. Gnotobiologic evidence for functions of the microflora. Erfahrungsforschung. 1965.;10:192-250.
- Matzker J and Steinberg A. Tonsillektomie und Leukämaie im Erwachsenen-Alter. Laryngologie, Rhinologie, Otologie. 1976:55(9).
- Miyakawa M and Luckey T, eds. Advances in germfree research and gnotology. 1968; Cleveland:Chemical Rubber Press.
- Nissle A. Darm-Dysbakterie und Krebs. Mschr Krebsbekämpfung. 1941:5.
- Nossal GJV and Mitchell JM. Thymus in relation to immunological tolerance. In: Ciba Fdn. Symposium. Thymus in immunity. 1966; London:Churchill.
- ----------. The cellular basis of immunity. Presented as the Harvey Lecture. 1968; March:New York Academy of Medicine.
- ----------. Antibody and Immunity. 1969. New York:Basic Books.
- Oeser H. Onkologische Radiologie, Erwartungen, Selbstzweck oder arztliche Aufgaben. 1977;Röntgenologen-Kongress:M,nster.
- Old LJ, Benacerraf B, Clarke DA, Carswell EA, Stockert F. The role of the reticuloendothelial system in the host reaction to neoplasia. Cancer Res. 1961;21:1281.
- Pischinger A. Über das vegetative Grundsystem. Physik Med Rehab. 1969;10:53-57.
- Pottenger FM and Simonsen DG. Heat Labile Factors Necessary for the Proper Growth and Development of Cats. J Lab Clin Med. 1939:25(6).
- Rössle R. Virchow's Archiv. 1930;288:781.
- Rubin BA. Carcinogen induzierte Toleranz. Prog Exper Tumor Res. 1964;5:217.
- Schade H. Die Physiol. Chemie in der inneren Medizin. 1923:Dresden.
- Schiephake E. Kurzwellen-Therapie. 1952;Stuttgart:Piscator.
- Schmid F. Staffelung der immunologischen Abwehrvorgänge. Deutsches frzteblatt. 1966;63:3009-3016.
- ----------. Allgemeine Immunologie. In: Handbuch der Kinderheilkunde, Band III. 1966;Berlin, Heidelberg and New York:Springer.
- Stanley WM. Die Beziehungen zwischen Viren und Krebs. Krebsarzt. 1957;6:307-320.
- Thomas L. In: Lawrence HS, ed. Cellular and humoral aspects of the hypersensitive states. Symposia of the Section on Microbiology of the New York Academy of Medicine. 1959;London Cassel:259.
- Warburg O. Über den Stoffwechsel der Tumoren. 1926;Berlin:Springer.
- Warning H. Die Ernährungsfrage und die Bedeutung der Pottengerschen Kaztenversuche. Hippokrates. 1954; 25:761-763.
- Wehrli F. Über die hämatogene. Oxydationstherapie. Hippokrates. 1958; 17:551-555.
- Zabel W. Die interne Krebstherapie und die Ernährung der Krebskranken. 1968; Bod Homburg v. d. H. :Bircher-Benner.
Published in
Explore! Volume 7, Number 6, 1997
Reprinted with permission of Explore Publications, PO Box 1508, Mt. Vernon, WA 98273, U.S.A.