Immunotherapy in Progressive Metastatic Cancer
Metastatic cancer: a fifteen-year follow up report by Dr. Josef Issels.

Immunotherapy in Progressive Metastatic Cancer a Fifteen-Year Survival Follow-up
by Josef Issels, M.D.
Ringberg-Klinik, Rottach-Egern, W. Germany
Published in the Clinical Trials Journal. London, 1970. 7, No. 3,
A Peer Reviewed Paper
Summary
A preliminary report on an unconventional method of treatment of advanced cancer is presented. Therapy is based on the concept that cancer is a chronic systemic disease, and consists of combined general and immunological treatment.
Combined treatment includes psychotherapy, the use of auto-vaccines for septic foci, treatment with organ extracts to restore function, hyperpyrexia and anti-tumor injections. Immunotherapy is by both active immunization with mycoplasma vaccine and passive immunization with antibodies from cancer cells.
Patients are treated only after they have undergone conventional surgery and radiation, and no conclusive results are claimed. From 750 cases who attended, 252 with a five-year survival were followed-up and of these 88 were studied for comparative investigation. Forty-two of the 252 (16.6 per cent.) were alive and fully fit for work five years after treatment, and of these 42, 39 were alive and well and showed no signs of cancer some 10 years later, making a total survival time of 15 years.
It is felt that the method should be further investigated and more details obtained to determine its possible value.
About 20 percent of all patients suffering from cancer, including cancer of the skin, live for five years or more after surgery, radiation and chemotherapy. Despite improvements in technique and chemotherapy, a decisive increase in this duration cannot be expected in the present state of knowledge. Only Burkitt's tumor, chorioepithelioma, and some forms of leukemia respond satisfactorily. For the remaining 80 percent of all other cancer patients, present methods of treatment cannot offer even a five-year remission, and in 1953 we showed the need for research for therapy for these cases who are either those with untreatable primaries, or who are relapsing due to the formation of secondary metastases, or who already have untreatable secondaries.
In view of this, research workers throughout the world postulate that new approaches should be considered in an attempt to improve this situation. Recent papers indicate that immunological mechanisms are receiving attention, as more virus and virus-like particles are found in the tumors of patients with cancer. Immunotherapy appears to be a promising, if not the only possible, way of treatment for such cases. 1, 2, 3, 4, 5
In 1953, we suggested the concept 6 that cancer must be understood and treated primarily as a chronic systemic illness of the whole body. The loss of resistance to cancer cells gives an acquired property for oncogenesis to the body which develops a long prediagnostic history for the condition. 6, 7, 8 Smithers 9 in 1962, suggested that cancer is a disease of organization and not a disease of cells; its field of study is science of organismal organization; it cannot be encompassed simply by cytology. Druckrey 10, in 1951, had put forward the hypothesis that the development and dissemination of cancer becomes possible by the weakening or loss of the natural resistance 11, 12, 13, 14, 15, 16 which destroys cancer cells which develop constantly and normally in a seemingly healthy organism. Natural resistance to cancer cells is incapacitated as a consequence of the complex summation of noxious substances and damage which has occurred sometimes a long time ago to the organism. These noxious substances lead to a complex chronic metabolic disturbance and prepare what has been described as a "tumor milieu."
For the past 20 years we have observed the effects of immunotherapy and general supportive treatment in about 6,000 cancer patients, 90 percent of whom have had progressive malignancy not responding to surgery, radiotherapy or chemotherapy.
Method
The following principles were used as a guide in the treatment of the 6,000 patients studied in this series.
- The mesenchymal system regulating and controlling the growth and distribution of normal cells, and the lysis of "abnormal cells" 17, 15 becomes disordered probably due to disturbances in the feed-back mechanism or in one of the cellular recognition or controlling factors. 18
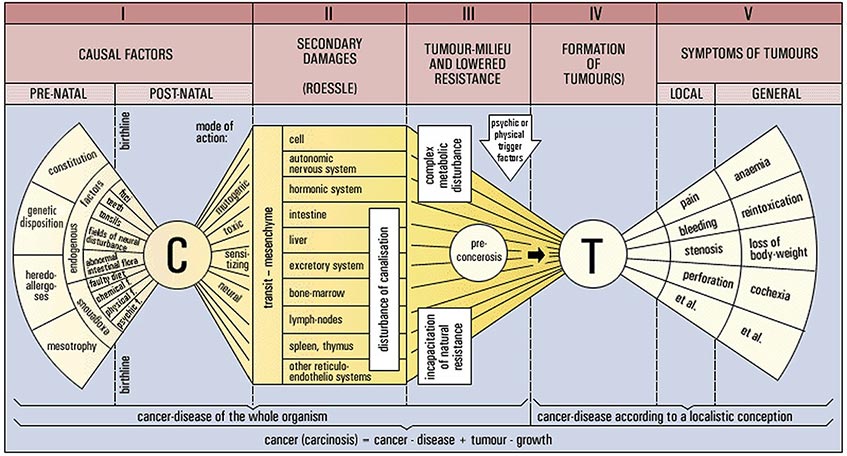
- A general chronic illness of the body without normal regulation of function leads to the permanent inability to destroy cancer cells and finally allows the formation of a tumor. 19, 17, 8The tumor is therefore merely a late stage symptom, accidentally triggered off, but able to exist and grow only in a bed already prepared for it. The "tumor milieu" is the result of secondary damage to organs and organ-systems 20, 21 affecting functional, regulative and humoral balance between organs and organ-systems with severe impairment of the system for the disposing of the products of lysed cells. 22, 23, 24 Secondary damage is sustained by causal factors of endogenous and exogenous origin. Causal factors may be found pre- and post-natally.
Thus the combined therapy of cancer consists of basic treatment of the body to eliminate its ability to develop abnormal cells, and other therapeutic procedures such as surgery, radiation, immunotherapy and chemotherapy which are necessary to attack the tumor itself (Figure 1).
Figure 1.
The basic treatment modified to suit individual patient's needs includes:
- (a) Elimination of all sizeable causal factors such as dental, alveolar and tonsillar foci, abnormal bacterial intestinal flora, fields of neural disturbance, faulty diet, exogenous factors, and psychic and emotional stresses. 25, 26, 27, 28, 29, 30
- (b) Desensitization of the body (already sensitized by causal factors) by (i) administration of "serum activator" (Theurer) to promote normal haemolysis of the patient's blood, (ii) injection of auto-vaccine prepared from teeth and tonsils extracts, (iii) injection of auto-vaccine from pathogenic coli bacteria, and (iv) administration of Spenglersane T, R, E, M, Om, K.
- (c) Treatment of secondary damage by means of substitution therapy to restore normal functions of organs by activation of cellular respiration, substitution of insufficient mesenchymal defensive properties, regeneration of organs and compensation of losses by the administration of organ extracts or organ hydrolysates.
Elimination of causal factors and the treatment of secondary damage as far as possible will favor the removal of tumor milieu, and tumors are further attacked by hyperpyrexia therapy-artificial induction of fever by administration of Pyrifer (Asta) or Vaccineurin (Sdmedica)– and by haematogenic oxidation therapy (HOT) as described by Wehrli. 31
Therapy to improve detoxification, i.e. the elimination of toxins resulting from oncolysis, and excretory canalization. i.e. the elimination of metabolic residues and toxins, is used in order to activate liver and kidney functions, the excretory actions of which are assisted by high fluid intake.
Elimination of the original tumor is encouraged by surgery, radiation, chemotherapy, enzyme therapy with lytic enzymes such as asparaginase, and immunotherapy by both active immunization with mycoplasma vaccine (Gerlach) and passive immunization with antibodies prepared from cancer cells.
Active immunization
The vaccine developed by Gerlach for the experimental treatment of malignant growths consists of a mixture of pure cultures of tumor mycoplasmae obtained after ultra filtration from tumor tissues of heterogenous malignant growths.
Cultivation is on a beef-agar medium containing glucose, peptone and horse-serum. 32, 33 Each mycoplasma strain extracted from tumors must be cultivated with numerous culture transfers over a long period of time before it can be used in a vaccine. Innocuity of each single strain as well as the complete vaccine must be tested on laboratory animals before administration to cancer patients is feasible. The concentrated broth culture, or dilutions thereof, well shaken, are injected intravenously or intramuscularly for weeks or months in doses depending on the patient's condition."34, 35
Passive immunization
Passive immunization is effected with standard preparations such as Centanit, Sarkogen and Lymphogran which induce formation of specific antibodies. Centanit is used in cases of all types of carcinoma; Sarkogen for all types of sarcoma. A special indication for Lymphogran is Hodgkin's disease (lymphogranulomatosis). Each ampoule contains 22 mg equivalent tumor antigens in 2.2 ml of normal saline. Subcutaneous injections of 0.2 to 0.3 ml are given every fifth to seventh day for at least three to six months. In particular cases passive immunization may be continued for years.
Clinical trials carried out by Gerlach using specific antiserum from horses immunized with cultures of human tumor mycplasmae have shown promising results and deserve further investigation.
By this basic treatment of a cancer patient (the host) it is possible to increase the effect of tumor-specific immunotherapeutic agents. This therapy improves the results of prior conventional treatment because it eliminates the otherwise unaffected tumor milieu and therefore the tendency for relapses or metastatic growth formation.
Our observations and experience in cases unsuccessfully treated, including the use of immuno-biological drugs, may be explained in that the principles of comprehensive treatment of the whole cancer-affected organism have not been observed.
Selection of patients
Patients were selected for statistical study according to the following conditions:
- The combined immunotherapy had to be carried through for at least two months as an in-patient.
- The diagnosis had to be established prior to admission by an independent physician and been verified microscopically by a pathologist.
- Patients had to be admitted for clinical treatment prior to May 1954.
- Patients had to have progressive tumor growth with metastases and relapses after termination of "normal", i.e. conventional treatment.
- Comparative numbers of cases had to be sufficient for statistical calculation.
- Comparative numbers from other hospitals, of patients treated by conventional cancer therapy were to be available for analysis.
- A further 370 patients were treated by general and immunotherapy following conventional treatment, and their five-year survival observed.
Results
The results of this treatment of progressive metastatic malignant growths over a period of five years were analyzed independently by Korthos and Audier in 1959 36; now 10 years later these patients have been reviewed again.
The 252 cases reviewed were a random sample of the 750 patients who had attended the clinic up to May, 1954. The diagnoses of their cancers are shown in Table 1. Of these 252 patients, 164 fulfilled conditions one to four only.
For comparative investigation and study 88 patients were selected, 48 of whom had cancer of the breast, 25 cancer of the uterus and 15 cancer of the colon and rectum, fulfilling conditions 1 to 6. Table II shows the five-year survival which was determined by Audier. 36
| Type | No. of Patients |
|---|---|
| Breast | 56 |
| Uterus | 42 |
| Stomach | 36 |
| Lung | 26 |
| Colon-rectum | 27 |
| Prostate | 3 |
| Ovarian | 7 |
| Urinary bladder | 3 |
| Liver | 5 |
| Pancreas | 3 |
| Pharyngeal | 3 |
| Larynx | 1 |
| Jaw | 5 |
| Other facial | 2 |
| Thyroid | 6 |
| Hypernephroma | 5 |
| Seminoma | 7 |
| Melanosarcoma | 3 |
| Other sarcoma | 12 |
| Total | 252 |
Of these 252 patients, 42 (16-6 percent.) were alive and fully fit for work five years later.
These 42 patients have again been followed up some 10 or more years after that study. In the interval three have died. Two died five and seven years after the completion of treatment respectively, from a late relapse of their cancer, and one died eight years later from infectious meningitis. The other 39 patients, who are alive and well, show no signs of cancer and are fully fit for work without any further follow-up treatment during the past 15 years. Other cases, including sarcomas, thyroid cancer, cancer of the epipharynx, etc., although living without relapse for more than five years after therapy, could not be taken into consideration because no comparative figures were then available. The types of cancer treated expressed as percentages, are shown in Table 111.
A preliminary study has also been made of a further 370 patients who were given the combined general and immunotherapy as a follow-up treatment shortly after surgery or radiation until 1960. Of these patients 322 (87 percent.) are alive and well after a period of five years with no relapses or detectable metastases to date. World statistics show a relapse rate of 50 percent. With this type of follow-up therapy the danger of recidivation is reduced to 13 percent.
Discussion
These results indicate the possibility, by using the combined general and immunotherapy technique, of producing prolonged remission in a significantly larger number of patients with progressive malignant disease than has so far been the general experience. Most of the survivors are alive and well 15 or more years after therapy.
Attention must be paid in the basic treatment not only to emotional and psychological problems of the patients who require intensive medical supervision, 12 but also to the restoration of all detoxifying mechanisms. Without sufficient detoxification, neither immunotherapy nor any other treatment will be successful. Often, by means of immunotherapeutic agents, tumors could be attacked and destroyed, but the patient would be lost because of his inability to eliminate oncolytic toxins. Some patients fail to respond to particular therapeutic procedures and alternatives have to be tried to produce the maximum response. Signs of fatigue after use of a particular immunizing agent may be observed, due to the formation of antibodies, so that it is essential frequently to change drugs.
| Site of Tumor | Cases Treated With Conventional + Immunotherapy |
Cases Received Immunotherapy only |
Reported Series, Conventional Treatment |
|||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Schwaiger, 1995 | Rossolec, 1995 |
Dalicho |
||||||||
No. Treated |
5-year Survivals |
No. Treated |
5-Year Survivals |
No. Treated |
5-Year Survivals |
No. Treated |
5-Year Survivals |
No. Treated |
5-Year Survivals |
|
| Breast | 48 |
6 |
21 |
3 |
35 |
2 |
20 |
1 |
--- |
--- |
| Colon-rectum | 15 |
4 |
8 |
4 |
17 |
3 |
--- |
--- |
--- |
--- |
| Uterus | 25 |
6 |
13 |
4 |
--- |
--- |
--- |
--- |
6 |
1 |
| Totals | 88 |
16 |
42 |
11 |
52 |
5 |
20 |
1 |
6 |
1 |
Five years after combined conventional and immunological therapies, 16 of these 88 patients (18.1%) were alive without relapse. Of the 88, 42 received immunotherapy only, 11 of whom were well five years later (26.2%). From the three reported series on conventional therapy, 7 of the 78 cases (9%) survived for five years.
| Type | % |
|---|---|
| Breast | 23.6 |
| Ovarian, uterine, vulva, vagina | 11.6 |
| Colon-rectum | 11.4 |
| Oesophagus and stomach | 9.2 |
| Sarcoma, melanosarcoma, endothelioma, cerebral | 9.1 |
| Larynx and lung | 8.8 |
| Urinary, bladder, kidney, adrenal | 5.1 |
| Prostate, testicular gland | 5 |
| Systemic disease (leukaemia, Hodgkin's plasmocytoma) | 4 |
| Gall-bladder, liver | 3.6 |
| Skin, penis, melanoma | 3.3 |
| Oral cavity, pharynx, other head areas | 2.5 |
| Primary unknown, metastases known Thyroid | 0.2 |
| Total | 100 |
Statistical evaluation of this type of treatment is extremely difficult. Patients are usually admitted after many different previous treatments (repeated surgery, irradiation, chemotherapy and therapy with hormones) so that classification of patients into specific groups with similar equal cancer or clinical condition is almost impossible.
The selection of patients was such that their lack of response to the standard methods of treatment was realized usually many months before they presented themselves, and metastatic spread of the cancer was evident in most of them. Some were in the terminal phase.
It was not possible to have controls in such a study, and every patient was given combined and general immunotherapy as early as possible once he presented to the clinic, to give the treatment the maximum chance of success.
As already outlined, cancer is a general systemic disorder and the various histological types of cancer, although relevant, are not primarily important in righting the whole condition. For therapy to be successful in removing the cause, the restoration of natural resistance is of decisive importance. Much more attention should be paid to the host and his general condition than has previously been done. This is not to say that surgery, radiation, chemotherapy and hormonal therapy are not useful, indeed they produce excellent remissions in appropriate patients and are an extremely useful adjunct to treatment.
In contrast to chemotherapy with its toxic side-effects as well as metabolic disturbance due to massive tumor destruction, it is worth noting that in individual cases optimal doses of immunotherapeutic agents cause an entirely uncomplicated resolution of the tumor if the excretory mechanisms are intact. In such cases the treatment appears to have affected the response of the system for dealing with malignant cells, and brought about spontaneous remission.
It has become apparent that metastases which are not detected radiologically can be located by pain in the appropriate area a few hours or days after administration of an immunotherapeutic agent. We believe, in contrast to other opinion, that this reaction is specific and allows the site of the original malignant tumor to be located, when secondary metastases are the only presenting symptoms. This is of particular clinical use in tracing and treating an unrecognizable primary tumor which has few metastases.
As an extension of our study, 1,000 extremely ill patients with rapidly progressive malignant growth and metastases to whom immunotherapy was considered to be of no immediate help, were given cyclophosphamide (Endoxana) at high dosage (50 to 80 mg/kg bodyweight) after the work of Blumenberg et al37, 38, 39 By this means fulminating tumor growths were halted so that subsequent immunotherapy was given a chance for further action. It is detrimental to give more than one or two massive doses of cyclophosphamide even well spaced apart because the immunological mechanisms become severely impaired so that subsequent immunotherapy does not produce a satisfactory response.
Randomized examples of cases, verified histologically, treated with basic and immunotherapy
Case I (336/59) – Male, born 12-4-1918
- History: May 1958, radical operation on primary tumor; post-irradiation 18,200 r only. November 1958, first local recidivation; after radiation 6,000 r apparent complete remission. April 1959, tumor-growth detected in abdomen; radiotherapy with 16,800 r OD with apparent complete regression.
- September 13, 1959 admitted to Ringberg Klinik as incurable, desolate case. Diagnosed progressive metastatic relapse of seminoma, left testicle, with cylindrical tumor size of goose egg in left hypogastric region.
- Therapy: Basic treatment and immunotherapy with Gerlach vaccine for nine months in 1959 and six weeks in 1960 as inpatient. Treatment continued during interval as outpatient.
- Result: Complete, persistent regression of seminoma for 10 years.
Case II (330/58) – Male, born 3-11-1921
- History: 1950, gastric ulceration. August 1958, incomplete resection of large gastric carcinoma which had already formed metastases in liver. No other specific treatment.
- 1958, admitted to clinic showing incompletely resected gastric carcinoma with progressive secondary growth.
- Therapy: Basic treatment and immunotherapy with Gerlach vaccine and other immunological drugs for 17 weeks in 1958-59 and for a further two weeks later in 1959 as inpatient; continued as outpatient during six-months' interval.
- Result: Complete, persistent regression for II years; patient is well and fully fit for work as University Professor.
Case III (491/68) – Male, born 3-6-1925
- History: November 1967, pre-operative radiation of malignant, degenerated birth mark on right upper arm; thereafter excision (melanoblastoma malignum) followed by intensive radiation. July 1968, metastases in regional lymph nodes. Post-operative radiation repeated, followed by partial removal and cobalt-60 radiation post-operatively.
- August 1968 admitted to clinic, diagnosed progressive incurable metastases of melanoma, with hard tumor, size of fist, in right axilla.
- Therapy: Basic treatment and immunotherapy with Gerlach vaccine for 12 weeks, followed by outpatient treatment for six months.
- Result: Complete, persistent regression of metastases; no relapse in two years.
Case IV (404/59) – Female, born 4-12-1911
- History: May 1954, radical mastectomy and post-radiation 4,200 r. December 1957, metastatic formations in ribs; radiotherapy. December 1958, local recurrence in scar; radio- and hormone therapies with apparent complete regression. September 1959, pulmonary metastases and again metastases in ribs.
- November 1959, admission to clinic; diagnosed incurable progressive third relapse of metastatic carcinoma of left breast, showing four metastatic rib fractures with tangerine-sized tumor in right lung, large pleural infusion and large ulcerating scar on right anterior chest wall.
- Therapy: Basic treatment and Gerlach vaccine for 14 months.
- Result: Complete, persistent regression of all metastases; observation period more than 10 years.
Case V (143/60) – Female, born 20-11-1900
- History: December 1959, exploratory laparotomy showed inoperable carcinoma of the sigmoid, adherent to uterus, adnexa, retroperitoneum and abdominal wall. Pre-natural anus made; cyclophosphamide therapy shortly followed by pulmonary embolism; then no further treatment.
- February 1960, admitted to clinic as incurable, progressive carcinoma of the sigmoid.
- Therapy: Basic treatment and Gerlach vaccine for 17 weeks.
- Result: Complete, persistent regression, observation period more than 10 years.
Case VI (312/60) – Female, born 7-5-1890
- History: September 1953, removal of spindle cell sarcoma from left shin bone and post-radiation. Summer 1958, local recurrence necessitating repeated surgery in March and August 1959, when diagnosis of sarcoma was again verified microscopically.
- October 1959, admitted to clinic, diagnosed incurable, progressive local recurrence of osteo-sarcoma, showing multiple sarcomatous tumors over a large area of post-operative skin-muscle-bone defect.
- Therapy: Basic treatment and Gerlach vaccine for eight weeks, then conservative outpatient treatment for several months; later, amputation of left leg.
- Result: No recurrence after more than 10 years.
References:
Editorial note: to facilitate publication, these references have not been checked.
- Wrba, H. (1969). "Neue Wege der Krebstherapie-Ausblick." Krebsarzt, 5, 281.
- Baruah, B. D. (1961). "Resistance to Cancer – an Immunological Approach." Current Medical Practice, 5, 192.
- Green, H. N. (1955). "Immunological Concept of Cancer." Annual Report of British Empire Cancer Campaign, 33, 202.
- Green, H. N. (1958). "Immunological Aspects of Cancer."
- Green, H. N. (1960). "The Immunological Theory of Cancer." Acta U. lnt. Cancer.
- Issels, J. (1953). Grundlagen und Richtlinien fuer eine Interne Krebstherapie, Hippokrates-Verlag, Marquardt & Cie, Stuttgart.
- Issels, J. (1954). "Ergebnisse und Erkenntnisse nach vierjahriger klinisch-interner Therapie beim inkurablen Krebs-Kranken." Hippokrates, 25, 16.
- Issels, J. (1956). "Gedanken zur Internen Behandlung von Tumor-Kranken." Hippokrates, 27, 16.
- Smithers, D. W. (1962). Lancet, 1, 443.
- Druckrey, H. (1950). "Die Grundprobleme der Krebsentstehung und des Krebswachstums." Med. Welt., 1, 1613, 1652.
- Caspari, W. Uber die Abwehrmassnahmen des Organismus gegen die Entstehung der Krebskrankheit, G. Thieme Verlag, Leipzig.
- Domagk, G. (1948-1950). "Die Bedeutung körpereigener Abwehrkräfte für die Ansiedlung von Geschwulstzellen." Zeitschr. Krebsforschung, 56, 247.
- Domagk, G. and Hackmann, C. (1953). "Die zusaetzliche Behandlung bösartiger Geschwülste durch Steigerung der tumorspezifischen Abwehr-Aktivität." Zeitschr. Krebsforschung, 59, 2.
- Meythaler, F. and Truckenbrodt, H. (1958). "Koerpereigene Abwehr und Krebs" Arztl Forsch., 12, 217.
- Pischinger, A. (1966). "Krebs und Abwehreinrichtungen des Organismus." Krebsarzt, 5.
- Schultz van Treeck, A. (1954). "Krebs und körpereigene Abwehr." Laryngologie, 33, 307.
- Fromme, A. (1953). Das Mesenchym und die Mesenchymtheorie des Carcinoms, Dresden/Leipzig.
- Burch, P. R. J. (1970). Nature, London, 225, 512.
- Bruda, B. W. (1931). "Die Bedeutung des Res fuer das Blastom-Wachstum." Zeitschr Krebsforschung, 34, 185.
- Roessle, E. (1950). Stufen der Malignitaet, Berlin.
- Roessle, R. (1923). Verh. Dtsch. Path. Ges., No. 19, 18.
- Kellner, G. (1963). "Die Wirkung des Herdes auf die Labilitaet des humoralen Systems." Osterr. Z. Stomatol., 60, 312.
- Warburg, 0. (1956). "Über die Entstehung der Krebszellen." A. Dietrich, Krebsforschung-Krebsbekämpfung, I, München; Berlin.
- Warburg, 0. (1947). Ideen zur Fermentchemie der Tumoren,Berlin.
- Issels, J. (1956). "Fokal-Infekt und Krebs." Deutsche Zahnaerztl. Zeitschrift, 11, 123.
- Kellner, G. (1967). "Nachweis der Herderkrankungen und ihrer Grundlagen." Therapiewoche, 15/24,.1267.
- Pischinger, A. (1961). "Über die vegetativen, insbesondere humoralen Grundlagen des Herdgeschenens." Arztl. Praxis, VIII, 5, 249.
- Pischinger, A. (1965). "Theoretische Grundlagen der Herderkrankung." Therapiewoche, 15/24, 1261.
- Schultz van Treeck, A. (1955). "Krebsdisposition und Wesenstypus." Dtsch. Ges. Wes., 10, 1273.
- Blumenberg, E., West, P. N. and Elis, F. W. (1954). "A Possible Relationship between Psychological Factors and Human Cancer." Journal of Psychosomatic Medicine, 227.
- Wehrli, F. (1955). "Neue Erfahrungen mit Krebskranken in der Haematogenen Oxidationstherapie." Cancer Therapy, 1.
- Gerlach, F. (1948). Krebs und obligater Pilzparasitismus. Urban und Schwarzenberg, Wien.
- Gerlach, F. (1970). "Zur Biologie der Mykoplasmen und ihre Beziehungen zu malignen Tumoren." Wiener Tieraertzl. Monatsschrift, in press.
- Gerlach, F. (1957). "Spezifisch bewirkte Latenz und Regression von Tumoren." Krebsarzt, 5, XII, 254.
- Gerlach, F. (1961). "Immunbiologische Studien bei malignen Tumoren und Haemoblastosen." Krebsarzt, 2, XIX, 54.
- Audier, A. G. (1959). "Immunotherapie metastasierender Malignome." Die Medizinische, No. 40, 1860.
- Blumenberg, F. W. and Scheef, W. 1968). Hochdosierte Cyclophosphatomide-BehandIung in Kombination mit Strahlentherapie bei Patienten mitfortgeschrittenen Tumorerkrankungen. Deutscher Krebskongress, Berlin.
- 38. Blumenberg, F. W. and Scheef, W. (1969). "Bericht ueber die 10. Wissenschaftliche Tagung des Deutschen Zentralausschusses für Krebsforschung und Krebsbekampfung." Fortschritte in der Krebsforschung, Schattauer-Verlag, Stuttgart.
- 39. Blumenberg, F. W. and Scheef, W. (1969). "Hochdosierte Cyclosphosphatomide-Behandlung in Kombination mit Strahlentherapie bei Patienten mit fortgeschrittenen Tumorerkrankungen." Med. Welt., 37, 2024.
Other Bibliography:
- Begg, R. W. (1958). "Tumour-Host Relations," Advances in Cancer Research, 5, 1.
- Dontenwill, W. (1955). "Über Spezifische Abwehrvorgaenge bei malignen Geschwuelsten." Verh. Dtsch. Ges. Path., 39, 337.
- Kollath, W. (1952). "Die Mesotrophie als physiologisches und klinisches Problem" Hippokrates, 23, 292.
Published in the Clinical Trials Journal. London, 1970. 7, No. 3, A Peer Reviewed Paper
Josef Issels, M.D.
Ringberg-Klinik, Rottach-Egern, W. Germany