Issels Holistic Integrative Approach to Cancer
Josef M. Issels, M.D., is remembered worldwide as the foremost pioneer of the holistic integrative approach to cancer.

Holistic Integrative Approach to Cancer: The Issels Treatment
by Ilse Marie Issels
Published in
Explore! Volume 9, Number 6, 2000
2000 copyright by Ilse Marie Issels, President,
Issels Foundation Inc.
Reprinted with permission of Explore Publications, Inc.
318 N. Rush Street, Prescott, AZ 86301
Josef M. Issels, M.D., is remembered worldwide as the foremost pioneer of the holistic integrative approach to cancer and chronic degenerative disease. He developed a comprehensive logistic treatment system which he first published in 1953 and administered to approximately 15,000 cancer patients in the hospital and clinic he founded in 1951 at Lake Tegernsee near Munich, Germany.
In 1970 the hospital was enlarged from 80 to 120 beds with extensive research facilities including a dental ward (for the diagnosis and treatment of focal infection), immunological and microbiological departments where various vaccines were developed. Programs included research on pleomorphism (Enderlein), microbes in oncogenesis, for example mycoplasma (Gerlach), autologous vaccines (Issels), mixed bacterial vaccines (Coley), darkfield microscopy, hyperthermia etc. The facility provided state-of-the-art medical care in a resort setting.
It was the first hospital of its kind, designed for the immunobiological treatment of cancer patients who had exhausted conventional treatments. Over 90% of all patients were suffering from progressive metastatic cancer, and too often in the terminal stage. The treatment of these patients posed new problems of therapy which had not been considered in classic cancer therapy, that is the treatment of the tumor alone.
The possibility of daily clinical observation and comparison of similar incurable cases for months at a time – the research at the bedside – permitted a new experience, centered on the body's natural defense, repair and regulatory mechanisms.
Dr. Issels summarized his conclusions from this experience in his holistic concept of the development of chronic degenerative disease and malignancy. It serves as the fundament for his comprehensive treatment strategy which attends to both the disease symptoms and the causes and preconditions for the development of these symptoms.
More Than Treatment of Just the Cancer Tumor
In the case of cancer, the treatment is not only directed at the malignant tumor, but also at the correction of the preconditions for the formation of the tumor. It aims for the restoration of the natural defense, repair and regulatory mechanisms of the cancer afflicted person as a whole.
Research has shown that every vertebrate organisms is constantly threatened by cancer cells whose formation is a daily occurrence. Not every newly produced cancer cell leads to a tumor, as the body possesses a natural defense system.
The system with the highest differentiation within the entity of the natural defenses is the cellular immune system. This has a homeostatic control function or immune surveillance according to the concept of Thomas. It is this system which differentiates between "self" and "non-self" and destroys alien or outlaw cells including cancer cells. Thus an intact immune system and intact regulation of physiological cell death (Villunger, Strasser) is capable of protecting the organisms from the development of a malignant tumor.
Dr. Issels differentiated between two causal complexes in the development of cancer, namely:
- the factors which induce the transformation of a normal cell into a cancer cell, and
- those factors which impair the immune and regulatory systems to an extent that they cannot prevent cancer cells from developing into a tumor
According to Buttersack, Eppinger, Schade and others the defense potential is a multi-layered structure of numerous, very different functional systems embracing virtually the whole body. During the decades of treating advanced cancer, Dr. Issels observed the synergistic effect of treatment modalities that comprise all the defense zones.
Table 1. Interaction Between the Neuro-Hormonal Control System and the Four Defense Zones.
Luckey and Schmid Differentiate between Four Successive Defense Zones:
- The adaptive "extracorporal defense zone". It consists of the physiological obligatory microflora on all epithelial surfaces with its autonomous defense function. It is responsible for the development of the "basic immunity of the organism" (Gordon, Luckey and Miyakawa). The functional integrity of the other defense zones can only be guaranteed by a healthy eubiotic microflora.The functional integrity of the other defense zones can only be guaranteed by a healthy eubiotic microflora.
- The constitutive "epithelial defense zone". It consists of all epithelial surfaces and performs defense, filtration, excretion and absorption (Carbonara, Crabbe, Heremans, Mitchison).The excretory function of this zone is of special importance for the elimination of metabolic and oncolytic toxins. A back flow of the waste products leads to a blockade of this system with all the consequences for the other zones, and thus to an impairment of the defense potential.
- The constitutive "lympho-reticular defense zone". It consists of the "lympho-epithelial system" with the thymus, the Waldeyer's tonsillar ring, the Peyer's patches, the "lympho-retothelial system" such as the white pulp of the spleen, the lymphatic centers, the white bone marrow and the storage endothelia. The importance of this zone has been shown by the research work of Alexander, Good, Hellstrom, Klein, Nossal, Old, and others.
- The constitutive "reticulo-histiocytary defense zone". It is the pluripotent mesenchyme which embraces almost half of the body weight. It is also called the regulatory ground system (Pischinger) with its various functions such as
- the transit function that intervenes between nerves, organ cells, blood, lymphatic and intestinal cells
- the homeostatic function
- the defense, detoxification and storage functions
These four defense zones are successive, are closely interrelated and – what is often neglected – they are under neuro-hormonal control. They do not only fulfill defense but also other vital functions.
The blockage of only one function of one of these zones, for example of the excretion belonging to the second zone, or even the blockage of the control system such as the diencephalon or the autonomous nervous system on its own, may contribute indirectly to a lowering of the defense potential.
The activities of the kybernetic synergism of the four defense zones are defined by some authors as the "big resistance". The resistance is a very complex mechanism which is not alone to be seen in the much discussed importance of the T-and B-lymphocytes. It is an accomplishment of the entire organism and therefore holistic.
To achieve optimal results treatment should cover all the defense zones including the control system whose importance has been shown by the research findings of psychoneuro-immunology.
The Issels Treatment comprises the person as a whole – body and mind. It is based on the concept of oncogenesis (Issels 1953) as outlined under table 2:
TABLE 2. Hypothesis of the Pathogenesis of Cancer.
Pre-and post-natal endogenous and exogenous factors (I) can lead by mutagenic, toxic, sensitizing and neural effects via the transit mesenchyme to secondary damage (Roessle) (II) to organs and organ systems as well as to functional disturbances of the neural, hormonal, excretory and defense systems.
Affects on the detoxifying and excretory systems deteriorate the endogenous environment or "milieu" and can lead to complex metabolic disturbances which are common to all chronic degenerative diseases and vary according to constitution and disposition.
Further constant influence of the causal factors and the persistence of secondary damages can impair the defense, repair and regulatory mechanisms to an extent that produces an imbalanced condition which, in the case of a genetic predisposition, can gradually develop into a "tumor-milieu (III). This constitutes a specific endogenous environment which provides the ideal medium for cancer cells, and microorganisms found in cancer, to thrive. From such pre-cancerous condition (III), when defense potency is lowered further, a malignant tumor may develop at the site of least resistance.
With the manifestation of the malignant tumor (IV) and its symptoms (V) the cancer disease enters the recognizable phase and conventional treatment starts with the weapons directed against the tumor and the cancer cells. However, the latent pathological processes preceding and producing the manifestation of the tumor, remain chronically active, even after elimination of the tumor; hence the high rate of recurrence after standard cancer treatment.
Standard cancer treatment is based on the "localistic" concept that views the malignant tumor as the beginning of a disease which progressively spreads throughout the body. This interpretation of cancer makes all measures of treatment concentrated on the tumor, seem causal and exhaustive. They are exhaustive in those cases in which the immune system is capable to recuperate after alleviation from the tumor load (Rubin).
The holistic concept views cancer as a systemic disease from the onset and the tumor as its late stage symptom. This concept, therefore, calls for a holistic strategy in order to achieve optimal treatment results.
The Issels Treatment Approaches to Cancer
Based on the holistic concept, the Issels Treatment has two main lines of approach to cancer which complement each other:
A. Treatment aiming at the removal or reduction of the tumor:
- Surgery
- Radiation
- Chemotherapy
- Hormone Therapy
- Hyperthermia and Other Non-Toxic Modalities
- Specific Immunotherapy.
B. Non-specific immunobiological basic treatment aimed at the restoration of the impaired defense, repair and regulatory functions of the tumor host.
The Basic Issels Treatment Program
The basic treatment is modified to suit each individual patient's needs. It includes:
1. Elimination of all sizable exogenous and endogenous causal factors that may lead to an impairment of the immune functions and may contribute to a transformation of
- a) Malnutrition to be replaced by a diet designed to meet the special needs of the individual cancer patient (Budwig, Gerson, Hildenbrand), with supplementation of vitamins, anti-oxidants, minerals, trace elements, enzymes;
- b) Abnormal bacterial intestinal flora to be normalized by diet and long term administration of coli cultures (Nissle) and probiotic cultures;
- c) Head foci of infection such as dental, alveolar and tonsillar foci to be removed by surgical intervention (Issels, Pischinger);
- d) Fields of neural disturbance to be neutralized by neural therapy (Huneke). Neural therapy and acupuncture are also administered in conjunction with conventional pain therapy;
- e) Hereditary allergoses and toxicoses to be treated by administration of specific colloids (Issels, Spengler);
- f) Environmental and occupational factors and addictions to be rectified by change of life style;
- g) Psychic stress to be relieved by psychological guidance, in single and group therapy, biofeedback, relaxation techniques, meditation, visualization;
- h) Physical therapy, hydrotherapy, breathing techniques, massage, lymph drainage etc.
2. Treatment of secondary damage and metabolic disturbance to restore normal function of organs by:
- a) Activation of cellular respiration by oxygen-ozone therapy in various forms, ultraviolet blood irradiation;
- b) Regeneration of organs and compensation of losses by administration of organ extracts or organ hydrolysates, (e.g. liver extract, thymus peptides);
- c) Therapy to improve detoxification, i.e. elimination of toxins resulting from oncolysis, and of metabolic residues by activation of liver and kidney function assisted by herbal extracts and high fluid intake, colon hydrotherapy, enemas;
- d) Enzyme therapy with proteolytic enzymes to eliminate immune suppressive factors such as immune complexes;
- e) Homeopathy, Isopathy.
3. Stimulation of immune response by:
- a) Hyperpyrexia, i.e. the injection of bacterial lypopolysaccharides, e.g. an autolysate of streptococci and bacterium prodigiosum (Coley), to raise body temperature up to 104 F. Hyperpyrexia fights latent infections, loosens regulative blockades, improves detoxification, damages cancer cells, temporarily raises the white blood count up to 30 - 40,000 and increases the release of interferon and interleukin. Over the past 40 years more than 100,000 applications were given in the Issels Hospital and Clinic in Germany without any adverse side effects.
4. Biological Response Modifiers, Autologous Vaccines.
The vaccines were developed in the Microbiological Department of the Issels hospital. From 1958 until 1973 Dr. Franz Gerlach was its director of research. He was a Professor of the University of Vienna, a researcher of the Pasteur Institute in Paris, well published in peer- reviewed medical journals, and internationally renowned for his research on mycoplasma and cancer. In the Issels hospital, thousands of mice served for a variety of studies, all of which confirmed that mycoplasma species can be causative or co-factors in oncogensis.
To quote Gerlach: "Mycoplasmas are, synergistically with other factors, essential and obligatory for oncogensis". For example, after cell free depot inoculation of mycoplasmas under the skin of 209 albino mice, 90.9% developed all types of malignancies, whereas of 600 control animals which were not inoculated, only 0,83% developed cancer.
Over the last hundred years, other scientists have as well associated microorganisms with oncogenesis. Recent research by reputable US scientists confirms the involvement of certain mycoplasma species in cancer (S.C.Lo et al.), the Gulf War Syndrome, Chronic Fatigue, Fibromyalgia and Rheumatoid Arthritis (Nasralla M., Nicolson G.L.et al.)
The mycoplasma vaccines developed in the Issels hospital were administered within the comprehensive treatment program.
Clinical observation showed that even in an advanced stage of malignant disease an immune reaction with complete long term remission can be achieved. The basic therapy seems to improve the immune reactivity of the body and the efficacy of applied tumor antigens. This may explain why tests in some cancer centers where only tumor antigens were given without the basic treatment, did not achieve the same results and led to such statements as "tumors of a certain size cannot be influenced immunologically".
The importance of the basic therapy can be seen in the fact that with its use immune paralysis simulated by intoxication could be eliminated within a few days and a sufficient immune response was achieved. In the Issels Hospital and Clinic it was repeatedly observed that by the elimination of foci, above all infected devitalized teeth and chronically infected tonsils, or with an active fever therapy, a blockade of the neuro-hormonal systems was broken.
Table 3 | Table 4 | Table 5 | Table 6
Especially during the first years of the development of the Issels Treatment, it became evident: specific immunotherapy was more effective when causal factors could be eliminated systematically and detoxification mechanisms and herewith the endogenous environment, the "milieu", could be normalized.
The normalization of the detoxification processes is an essential part of basic therapy. This is generally ignored in research and practice. Despite all efforts, even today many patients are lost who respond well to the tumor antigens, but who are not able to excrete the products of tumor lysis. Without sufficient detoxification neither immunotherapy nor chemotherapy will achieve long term results.
In patients with a rapidly growing tumor who cannot expect immediate help from long term immunotherapy, the latter is combined with chemotherapy according to the morphology of the tumor. Thus the progression of the tumor growth can be stopped and the patient gains time to respond to immunotherapy.
In qualified cases, cautious short term administration of chemotherapy avoids the severe immune suppression associated with prolonged use of these drugs (Frei). Experience of 40 years has shown that chemotherapy combined with basic therapy, has less toxic side effects, and in special cases, when given in lower than the standard doses, it has the same cytotoxic effect. Thus many patients can be helped who would die, if only one of these therapies were used.
It has also been observed that through comprehensive immunobiological treatment alone or in combination with chemotherapy, a variety of inoperable tumors can be rendered operable. Blocked ureters or gall bladders can be freed, making it possible to continue treatment of patients who would otherwise be lost.
A decisive improvement of cure rates can be achieved through comprehensive immunotherapy as follow-up treatment shortly after standard treatment, such as surgery, radiation and chemotherapy. The restoration of the immune functions can reduce the incidence of recurrence from about 50% (World Statistics) to 13% by combined conventional treatments and comprehensive immunotherapy.
Josef M. Issels, M.D. reported in "Immunotherapy in Progressive Metastatic Cancer, A Fifteen Year Survival Follow-up" 1970, Clinical Trials Journal, 7(3): 357-366, London, a peer reviewed paper, that of 370 patients with various types of cancer who were given immunological treatment shortly after surgery or radiation therapy, 322 (87%) were alive and well after five years without recurrence or detectable metastases.
An independent statistical study by A.G. Audier, M.D., University of Leiden, Holland, "Immunotherapie Metastasierender Malignome" , 1959, Die Medizinische 40: 1860-64, Stuttgart, a peer reviewed paper, reported a 16.6% cure rate of histologically verified metastatic malignomas by the Issels comprehensive immunotherapy. The study comprised 252 patients with various types of cancer after all conventional methods were exhausted (World wide cure rate is 2%).
John Anderson, M.D., Teaching Professor at King's College Hospital, London, reported 17% cures of histologically verified metastatic malignomas by the Issels comprehensive immunotherapy. The independent randomized study comprised 570 patients with various types of cancer after all conventional methods were exhausted (General Practitioner, 1971 : 15-16, London).
Table 7 | Table 8 | Table 9 | Table 10 | Table 11 | Table 12 | Table 13
Surgery, Chemotherapy or Radiation May Still be Recommended
It is not the purpose of immunotherapy to replace surgery, radiation and chemotherapy. These "localized" treatments have their place within the integrative approach to cancer. On their own, however, they cannot be expected to be the answer to a chronic systemic disorder, although they have given their utmost in removing its symptom, the tumor.
Therefore, interdisciplinary collaboration should no longer be subject to the primacy of surgery, radiation and chemotherapy under the exclusion of immunotherapy.
It is the integrative approach to cancer based on the holistic concept that will bring physicians and scientists closer to their goal: A Cure for Cancer.
About the Author

Ilse Marie Issels was the wife and for 40 years the closest collaborator of Josef M. Issels, M.D. (1907 – 1998). His continuous research until his recent death enabled him to integrate advanced state-of-the-art technologies into his comprehensive treatment program.
Mrs. Issels follows this strategy. As the president of the Issels Foundation she carries on Dr. Issels legacy. Mrs. Issels is a consultant to hospitals and clinics implementing the Issels Treatment.
References:
- Alexander P. In: Prog Emp Tumour Res. 1968; Basel and New York; Karger; 10:22.
- Anderson J. General Practitioner. 1971; March 26:15-16.
- Audier AG. Immunotherapie metastasierender Malignome. Die Medizinische. 1959; 40:1860-64.
- Bahnson CB, et al. Die Bedeutung des eigenen Abwehrvermögens bei der Ätiologie maligner Tumoren. Ann NY Acad Sci. 1966; 125:827.
- Bauer KH Das Krebsproblem. 1963; Berlin; Springer.
- Boyse EA, Old LJ. In: Smith RT, Landy M, eds. Immune Surveillance. 1971; New York: Academic Press.
- Brunner KW, Nagel GA. Internistische Krebstherapie. 1976; Berlin:Springer.
- Burnet M. Immunological Surveillance. 1970; Oxford:Pergamon.
- Buttersack F. Latente Erkrankugnen des Grundgewebes. 1912:Stuttgart.
- Coley-Nauts H, Swift WE, Coley BL. Treatment of Malignant Tumors by Bacterial Toxins. Cancer Research. 1946; 6:205-215
- Crabbe PA, Carbonara AO, Heremans F. The normal human intestinal mucosa as a major source of plasma cells containing yA-immuno-globulin. Lab Invest. 1965; 14:235
- Danopoulos ED, Danopoulou IE. Eleven years experience of oral urea treatment in liver malignancies. Clin Oncol. 1981 Dec; 7(4):281-9.
- Danopoulos ED, Danopoulou IE. The effects of urea treatment in combination with curettage in extensive lip cancers. J Surg Oncol. 1982 Mar;19(3):127-31.
- Enderlein G. Bakterien-Cyclogenie. 1925: Berlin:Walter de Gruyter.
- Eugster J, Hess VF. Die Weltraum-Strahlung und ihre biologische Wirkung. 1940:Zurich.
- Frei E. Combination Cancer Therapy. Cancer Research. 1972; December; 32:2593-2607.
- Gerlach F. Krebsund obligater Pilzparasitismus. 1948;Vienna:Urban and Schwarzenberg.
- ----------.Oncogenese unter Beteiligung von Mykoplasmen. Wiener Medizinische Wochenschrift Supplement No. 26(4/1975)
- Gerson M. No cancer in normal metabolism: Outcomes of a specific therapy. Med Klin. 1954:49(5):175-179: Cancer, a problem of metabolism. Med Klin. 1954: 49(26):1028-1032; On the medications of cancer management in the manner of Gerson. Med Klin. 1954; 49(49):1977-1978.
- Good RA. In: Bergsma D. Immunologic deficiency diseases in man. 1968; New York; Nat'l Fdn March of Dimes:355.
- ----------, Finstad J. Essential Relationship between the lymphoid system and immunity. In:Miescher PA and Graber P, eds. Immunopathology V. 1967.
- Hellström KE and Hellström I. Advan Cancer Res. 1969; 12:167-223.
- ----------. Immunity of Neuroblastoma. Annual Review of Medicine. 1972:23.
- Helm F and Klein E. Arch Dermat. 1965:91(124).
- Hildenbrand GLG, Hildenbrand C, Bradford K, Cavin S. 5 year survival rates of melanoma patients treated by diet therapy after the manner of Gerson. Alt Ther Health. Med. 1995; I(4):29-37.
- Huneke F. Das Sekundenphänomen. 1956; Ulm and Heidelberg:KF Haug.
- Issels JM. Therapeutische Richtlinien bei inoperablenmalignen Tumoren. Vortrag auf dem 5. Berchtesgadener Kurs f, r Ganzheitsmedizin. 1952. In: Zabel W. Ganzheitsbehandlung der Geschwulstkrankheiten. Stuttgart: Hippokrates.
- Issels JM. Cancer: A Second Opinion. New York, Avery Publ. 1999
- ----------. Ergebnisse und Erkenntnisse nach vierjähriger klinisch-interner Therapie beim inkurablen Krebskranken. Hippokrates. 1954; 25 u. Bildbeilage:514-529.
- ----------. Gedanken zur Internen Behandlung von Tumorkranken. Hippokrates. 1956; 27 u. Bildbeilage:173-180.
- ----------. Fokalinfekt und Krebs. Dtsch Zahnärztl Zeitschr. 1956;11:123-131.
- ----------. Mehr Heilungen von Krebs. 1972; Bad Homburg v. d. H. :Helfer.
- ----------. Cancer: A Second Opinion. 1975; London:Hodder and Stoughton.
- ----------. Immunotherapy in progressive metastatic cancer. Clinical Trials Journal. 1970;7(3):357-366.
- Klein G. Tumor Antigens. Ann Rev Microbiol. 1966; 20:233-252.
- Lewis MG, Lewis, TM. Einfluss humoraler Immunmechanismen auf die Metastasierung menschlicher Tumoren. M, nch Med Wchnschr. 1977;28(43):119.
- Lo SC et al. Tsai S, Wear DJ, Shih W, Lo SC. Mycoplasmas and oncogenesis: persistent infection and multistage malignant transformation. 1995, Proc Natl Acad Sci USA; 92(22): 10197-201.
- Luckey TD. Germfree life and gnotobiology. 1963; New York and London:Academic Press.
- ----------. Gnotobiologic evidence for functions of the microflora. Erfahrungsforschung. 1965.;10:192-250.
- Matzker J and Steinberg A. Tonsillektomie und Leukämaie im Erwachsenen-Alter. Laryngologie, Rhinologie, Otologie. 1976:55(9).
- Miyakawa M and Luckey T, eds. Advances in germfree research and gnotology. 1968; Cleveland:Chemical Rubber Press.
- Nasralla M, Haier J, Nicolson GL. "Multiple mycoplasmal infection detected in blood of Chronic Fatigue and Fibromyalgia Syndrom patients. 1999, Eur.J.Clin. Microbiol.Infect.Dis. 18:859-865.
- Nissle A. Darm-Dysbakterie und Krebs. Mschr Krebsbekämpfung. 1941:5.
- Nossal GJV and Mitchell JM. Thymus in relation to immunological tolerance. In: Ciba Fdn. Symposium. Thymus in immunity. 1966; London:Churchill.
- ----------. The cellular basis of immunity. Presented as the Harvey Lecture. 1968; March:New York Academy of Medicine.
- ----------. Antibody and Immunity 1969. New York:Basic Books.
- Oeser H. Onkologische Radiologie, Erwartungen, Selbstzweck oder arztliche Aufgaben. 1977;Röntgenologen-Kongress:M,nster.
- Old LJ, Benacerraf B, Clarke DA, Carswell EA, Stockert F. The role of the reticuloendothelial system in the host reaction to neoplasia. Cancer Res. 1961;21:1281.
- Pischinger A. Über das vegetative Grundsystem. Physik Med Rehab. 1969;10:53-57.
- Pottenger FM and Simonsen DG. Heat Labile Factors Necessary for the Proper Growth and Development of Cats. J Lab Clin Med. 1939:25(6).
- Rössle R. Virchow's Archiv. 1930;288:781.
- Rubin BA. Carcinogen induzierte Toleranz. Prog Exper Tumor Res. 1964;5:217.
- Schade H. Die Physiol. Chemie in der inneren Medizin. 1923:Dresden.
- Schiephake E. Kurzwellen-Therapie. 1952;Stuttgart:Piscator.
- Schmid F. Staffelung der immunologischen Abwehrvorgänge. Deutsches frzteblatt. 1966;63:3009-3016.
- ----------. Allgemeine Immunologie. In: Handbuch der Kinderheilkunde, Band III. 1966;Berlin, Heidelberg and New York:Springer.
- Stanley WM. Die Beziehungen zwischen Viren und Krebs. Krebsarzt. 1957;6:307-320.
- Thomas L. In: Lawrence HS, ed. Cellular and humoral aspects of the hypersensitive states. Symposia of the Section on Microbiology of the New York Academy of Medicine. 1959;London Cassel:259.
- Villunger, Strasser A. Does "Death receptor" signaling play a role in tumorigenesis and cancer therapy? 1998; Oncol.Res.10(11-12): 541-50.
- Warburg O. Fber den Stoffwechsel der Tumoren. 1926;Berlin:Springer.
- Warning H. Die Ernährungsfrage und die Bedeutung der Pottengerschen Kaztenversuche. Hippokrates. 1954; 25:761-763.
- Wehrli F. Fber die hämatogene. Oxydationstherapie. Hippokrates. 1958; 17:551-555.
- Zabel W. Die interne Krebstherapie und die Ernährung der Krebskranken. 1968; Bod Homburg v. d. H. :Bircher-Benner.
Reference Tables
Table 3.
Consequences of Head-Foci on the body's regulatory and repair functions which over time can lead to an impairment of the defense potential.
Table 4.
Interrelation between head-foci and tumor demonstrated by the measurement of the infrared emission above devitalized teeth and infected tonsils. After extraction of devitalized (root canal treated) teeth and tonsillectomy and subsequent neural therapy (procain injections into the scars), the infrared emission completely disappeared. Measurement by infrared toposcope (Schwamm and Reh)
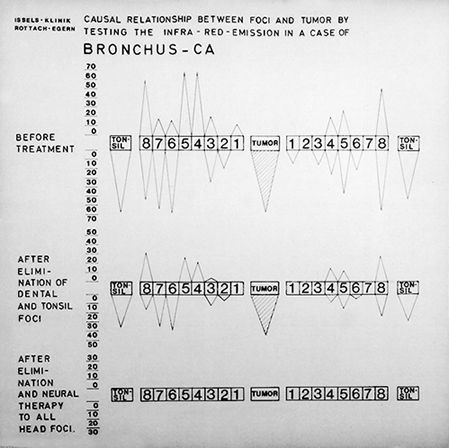
Table 5.
Example of breaking through a blockade of the neuro-hormonal control system by administering hyperperexia or active fever treatment (Coley's mixed bacterial vaccines). A fever chart of the Ringberg-Klinik, Dr. Issels' hospital in Germany, demonstrates the course of the Issels treatment for 4 weeks of a boy suffering from an oligodendroglioma who had not responded to conventional treatments and was considered in terminal stage. He received hyperpyrexia and developed fever for several hours with a peak of 104. Before the fever treatment he had up to 8 epileptic seizures daily, which is marked on the fever chart with flashes. During the rise of the temperature and its peak he had seizures, but on the following day the seizures subsided to one seizure once per week during the fever treatments. Three months of intensive inpatient treatment were followed by 6 months of outpatient treatment. Complete long term remission of the brain tumor was achieved through comprehensive immunotherapy without any conventional treatment.
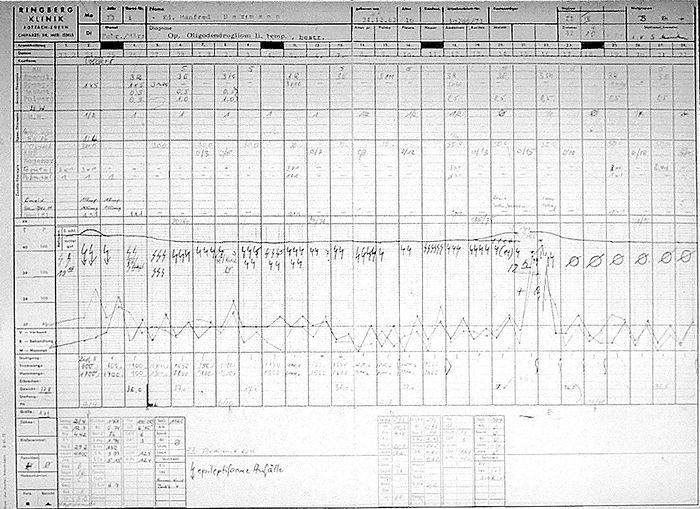
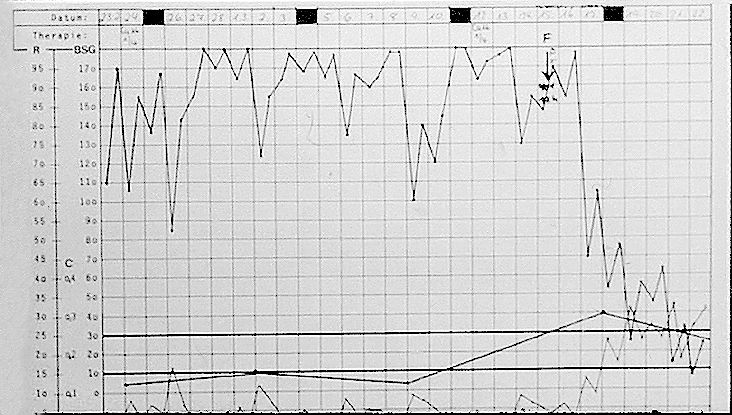
Table 6.
Measurement to objectivate the reactivity of the sympathicotonic and para-sympathicotonic systems. The correlation between the polarization capacity C and resistance R of the skin on the one hand and the sympathicotonic and para-sympathicotonic reactivity on the other hand, can be utilized to evaluate the condition of the neuro-hormonal control systems. It is one tool to monitor the patient's response to treatment on a day by day basis. For example in Table 5, the chart below the fever chart shows a blockage of the neuro-hormonal control which cannot be seen from the temperature and pulse. Judging from previous experience it was assumed that due to this freeze of regulations, the patient did not respond to any treatment. The fever achieved a release of this freeze and subsequent Issels treatment (comprehensive immunotherapy) was successful.
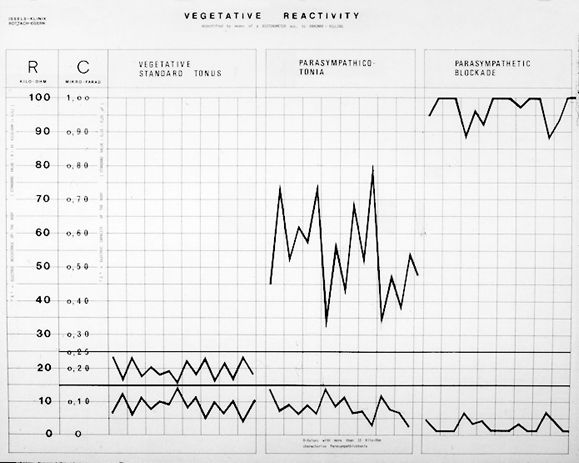
Table 7.
Demonstration of the enhancement of the immune mechanisms by hyperpyrexia, the active fever treatment. Count of the leukocytes 24 hours after fever treatment showed a temporary increase from 4000 to 10,000 and from 9,000 even up to 40,000, whereas passive hyperthermia did not increase the white blood count<.

Table 8.
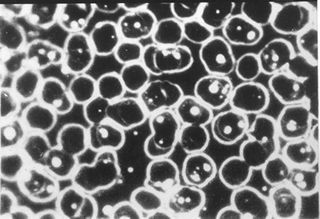
Examination under the darkfield of blood stained by the modified gram stain after the method developed by von Brehmer. This slide shows blood of a healthy person. Erythrocytes look quasi normal in shape and there are no inclusions.
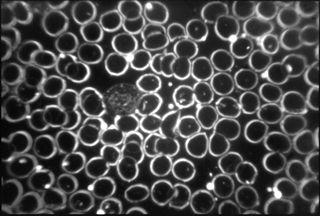
Table 9.
This slide shows blood stained by the modified gram stain after v. Brehmer and represents blood as seen with 90% of cancer patients. Von Brehmer and other researchers interpret the inclusions within the erythrocytes as microorganisms which are thought to be causal or co-factors in oncogenisis. In Dr. Issels' hospital the patients' blood was examined under the darkfield on weekly basis or, depending on individual needs, more often. It was observed that during successful cancer therapy, blood as represented in table 9 could be reverted to the condition as seen. It was observed that during successful cancer therapy, blood as represented in table 9 could be reverted to the condition as seen in table 8. Table 9 shows a magnification of the blood sample.
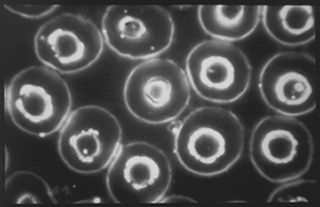
Table 10.
Blood of a sarcoma patient who had undergone preparatory Issels treatment before radiation (sample stained after the method of v. Brehmer).
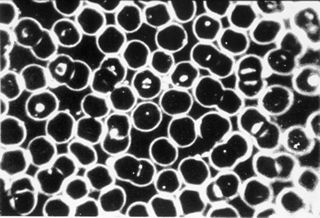
Table 11.
Blood of the same sarcoma patient 6 hours after the first radiation treatment of 250 r (sample stained after the method of v. Brehmer).
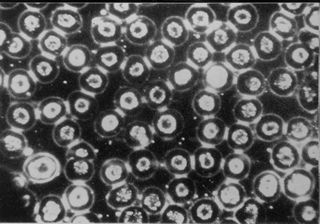
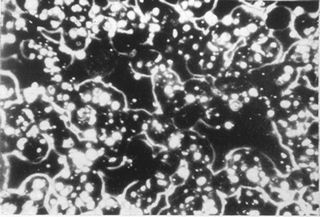
Table 12.
Blood of the same sarcoma patient 64 hours after the fifth radiation treatment (sample stained after the method of v. Brehmer).
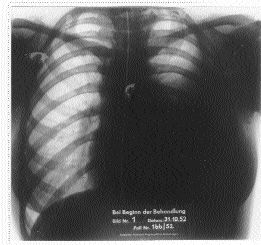
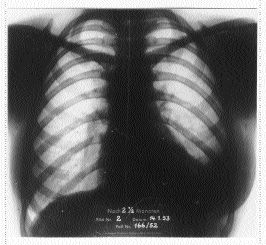
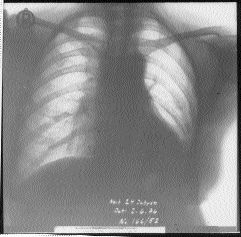
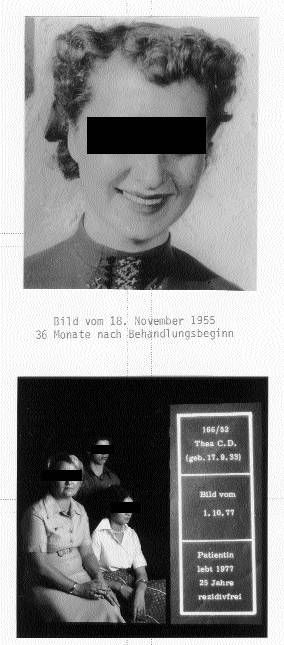
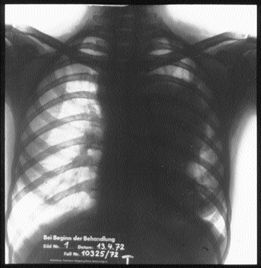
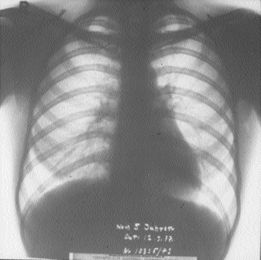
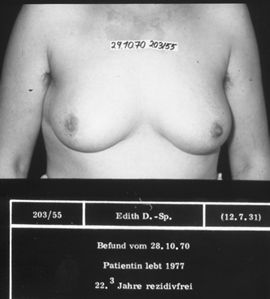
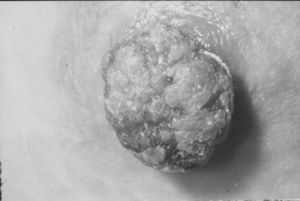
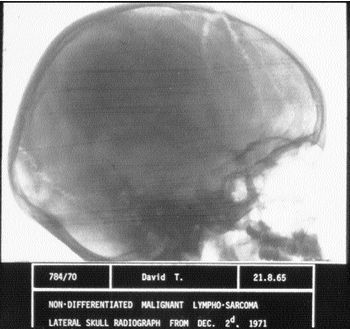
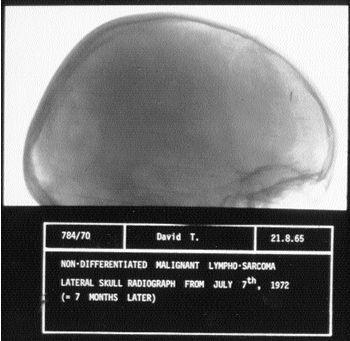
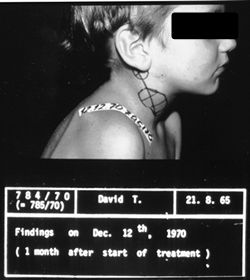
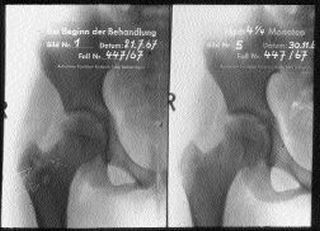
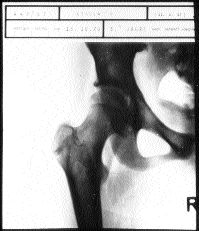
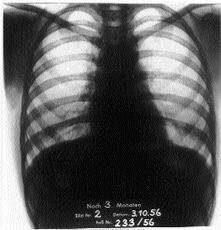
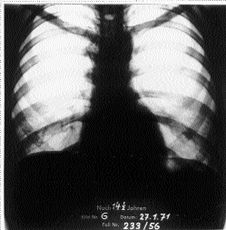
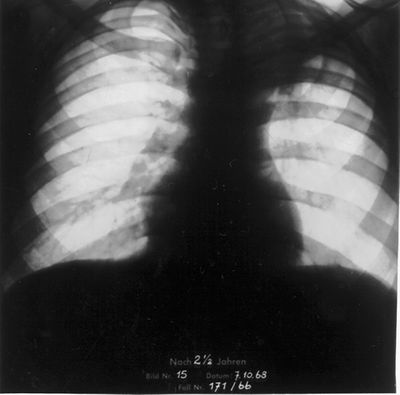
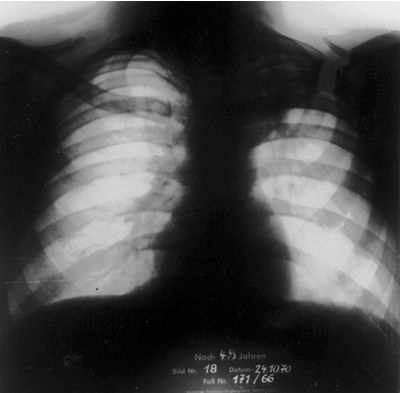
Representative Cases
Cases that demonstrate complete long term remission due to the Issels Treatment without conventional therapy or in combination with conventional therapy
|
|
|---|
 |
 |
|---|
 |
 |
|---|
 |
 |
|---|---|
 |
 |
 |
 |
|---|
 |
 |
|---|
 |
|---|
 |
|---|
 |
 |
|---|
 |
 |
|---|
 |
 |
 |
|---|
Published in
Explore! Volume 9, Number 6, 2000
2000 copyright by Ilse Marie Issels, President,
Issels Foundation Inc.
Reprinted with permission of Explore Publications, Inc.
318 N. Rush Street, Prescott, AZ 86301